
Guidelines recommend routinely assessing HHV-6 viral load, but not antiviral treatment when HHV-6 reactivation identified.
Drug reaction with eosinophilia and systemic symptoms (DRESS) is a rare drug hypersensitivity reaction. It always affects the skin, but it also can affect many other organs—often including the liver and kidney and sometimes the lungs, heart, and nervous system. Severity ranges from mild to severe, even life-threatening.
HHV-6 (primarily HHV-6B) is frequently reactivated in people with DRESS. The same is true of CMV, EBV and HHV-7, although studies of blood suggest that HHV-6B is by far the most frequently reactivated herpesvirus. (Zhu 2023)
Reactivation of HHV-6 in blood typically is detected 2-4 weeks after the onset of symptoms. Therefore, it is generally thought that the virus is unlikely to be a cause of DRESS. Instead, it appears more likely that inflammation precipitated by the drugs leads to the pathology of DRESS also encourages reactivation of HHV-6.
Recently, however, HHV-6 was found to be reactivated in the skin of people with DRESS shortly after the onset of symptoms and typically before reactivation is noted in the blood (Marcombes 2023). This raises the possibility that the reactivation of the virus at an earlier stage of the disease than previously noted might somehow “prime” the immune system to develop a hypersensitivity reaction to the offending drugs, as suggested by the expert panel and others (Pichler 2023).
Whether the reactivation of HHV-6B contributes to the onset of DRESS, or not, there is strong evidence that it increases the severity and duration of the illness (Zhu 2023).
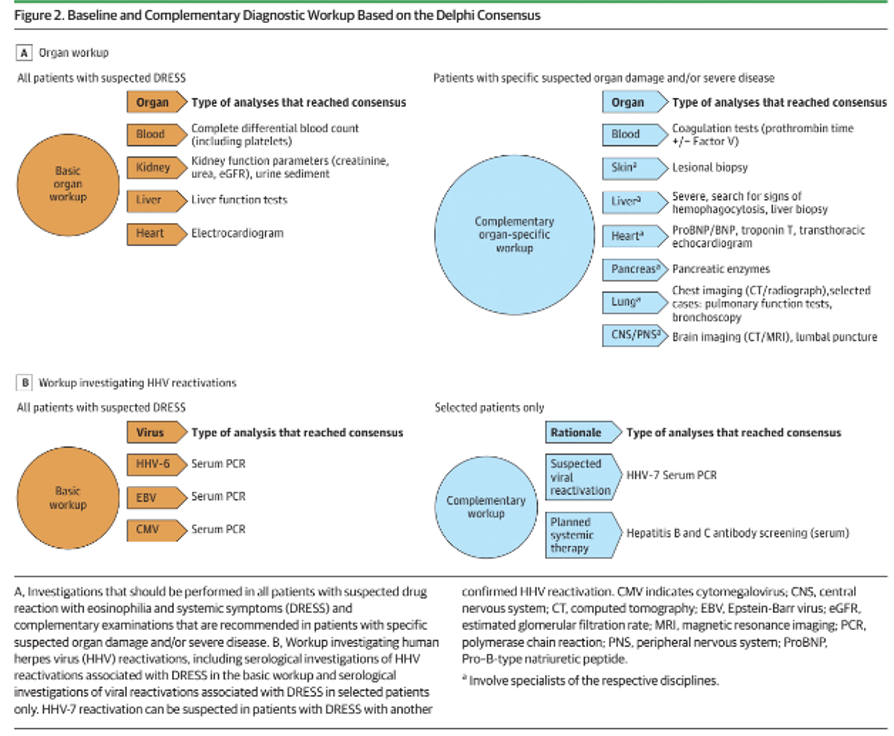
An international panel (21 countries and 4 continents) of 54 experts met to develop evidence-based guidelines for the diagnosis and treatment of DRESS. They used the Delphi method to develop the guidelines, a widely used and well-established method for reducing undue influence in the group process by individuals of unusual renown or with exceptionally forceful personalities. The experts were given 11 specific topics to consider and were presented with an extensive literature review on each topic.
The process led the panel to issue the following guidelines:
- EBV, CMV, and HHV-6 viral loads should be measured for all patients with suspected DRESS. The same was not recommended for other herpesviruses, including HHV-7, due to lack of evidence they were frequently reactivated in DRESS, or because good technologies were not widely available to diagnose reactivation.
- Ganciclovir or valganciclovir should be considered to treat a high CMV viral load: this was the first guideline recommendation of any antiviral therapy in DRESS, although some individual investigators have suggested it in the past.
- When DRESS is refractory to first-line therapy with corticosteroids, treatment with IVIG or cyclosporine should be considered, as should treatment with IL-5/IL-5R antibodies.
- Patch tests to assess allergies to various substances should be considered.
The guidelines are summarized in the figure, below.
These guidelines represent the first formal recommendation that HHV-6 viral load measurements should be made in people with DRESS. Although the guidelines do not recommend antiviral therapy for people with DRESS and high HHV-6 viral load, given that HHV-6B is the most frequently reactivated herpesvirus and that antiviral therapy for HHV-6 is recommended in people with HHV-6-associated illnesses (e.g., encephalitis) following hematopoietic cell transplantation, individual clinicians may continue to prescribe antiviral therapy in such cases.
Unfortunately, no mention was made of published pathology studies demonstrating that HHV-6B infection can cause severe organ damage in DRESS/DIHS patients (Miyashita 2016, Charnot-Katsikas 2016).
Clinical trials are urgently needed to evaluate the efficacy of antiviral treatment in DRESS patients with HHV-6B reactivation.
Read the full article: Brüggen 2023