A group from University of Chicago Medicine urged physicians to consider testing for HHV-6 in cases of unexplained liver failure in immunocompetent patients, especially those diagnosed with hypersensitivity disorders, citing evidence from past studies as well as their own recent case experience.
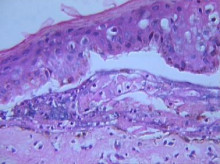
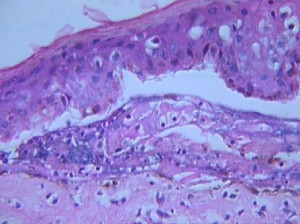
Led by pathologist Angella Charnot-Katsikas, the case report described a previously healthy woman who developed toxic epidermal necrolysis (TEN) and then succumbed to fulminant hepatic failure from HHV-6. The patient had a high viral load as well as post-mortem biopsy with immunohistochemistry demonstrating actively replicating HHV-6 virus.
This is one of the few studies to investigate viral infection as a possible cause of organ failure in a drug hypersensitivity case. Another recent report found HHV-6 to be the cause of kidney failure in a DIHS case (Myashita 2016). Both case reports were done post-mortem.
The 44-year old patient presented with fever, sore throat, abdominal pain, vomiting, facial and hand edema, diffuse macular and pruritic rash, ascites and hepatosplenomegaly. HHV-6 viral load was 250,000 copies/mL, which dropped to 12,574 copies/mL after ganciclovir administration. A skin biopsy was consistent with TEN, and the patient also suffered from ischemic infarctions and hemophagocytosis.
Post-mortem PCR was positive for HHV-6B, and a droplet digital PCR excluded ciHHV-6. The liver showed severe necrotizing hepatitis but no viral inclusions. Immunohistochemistry analysis using an HHV-6 monoclonal antibody showed intense immunoreactivity in both the skin and liver glandular epithelium.
Although the authors concluded that HHV-6 was the most likely culprit, they suspected that interaction of other herpesviruses (EBV and CMV) might have contributed to a more severe disease course in this patient.
The authors point out that in a study of 15 patients with acute liver failure of unknown etiology, 80% of the livers had evidence of HHV-6, compared to only a few cases in control livers. There have been a significant number of case reports of HHV-6 fulminant hepatitis in immunocompetent patients published in the past (Asano 1990, Harma 2003, Harma 2013, Ishikawa 2002, and Mendel 1995). One study (Ishikawa 2002) detected HHV-6 in patients with Non-A, B, C (NABC) fulminant hepatitis, but not in controls with HBV hepatitis; HHV-6 was also found to be a more common cause of fulminant hepatitis than CMV or EBV.
Although there have been occasional reports of HHV-6 reactivation associated with TEN (Teraki 2008, Watanabe 2013), it is usually associated with drug hypersensitivity (DIHS), and in fact HHV-6 is one of the criteria for diagnosing Drug-induced hypersensitivity syndrome (DIHS) in Japan. In this case report, eosinophilia and atypical lymphocytosis were not present, and the skin biopsy was more consistent with TEN. The onset of these symptoms was very rapid, unlike typical drug hypersensitivity cases that appear several weeks after an inciting drug.
HHV-6 has been associated with portal necrosis in transplant recipients with reactivated HHV-6 and liver failure, but biopsy analysis may be required because HHV-6 DNA is often at normal levels in the peripheral blood in spite of active infection in the liver (Buyse 2013).
HHV-6 reactivation has occasionally been reported in association with hemophagocytosis in primary infections (Marabelle 2010, Takagi 1996), healthy adults (Tanaka 2002) and in liver transplant patients (Dharancy 2008).
In this case, there was evidence for CMV and EBV reactivation as well. According to a Japanese study of 62 patients with hypersensitivity syndromes, EBV is active in about half of patients with SJS but less than 20% of patients with TEN and less than 10% of patients with DIHS/DRESS. CMV occurred in 22% of those with SJS/TEN and 17.6% of those with DIHS/DRESS, whereas HHV-6 occurred in all patients with DIHS/DRESS and none of the patients with SJS/TEN. Furthermore, they determined that steroids increased the viral load significantly for HHV-6, but not for CMV or EBV (Ishida 2014).
Some have proposed that patients with drug hypersensitivities should be treated with a combination of both an antiviral and prednisone (Moling 2012, Descamps 2013).
For more details, read the full paper here.
See also our pages on HHV-6 & Liver Disease and HHV-6 & Hypersensitivity (DRESS, DIHS).