
As diagnostic techniques have improved, DNA from a number of viruses has been detected in myocardial tissue from people with myocarditis and dilated cardiomyopathy (DCM). A high prevalence of HHV-6 (43.7%) in archival tissue from the explanted heart of pediatric patients with DCM has been reported previously (Comar 2009).
Bibhuti Das of Texas Children’s Hospital, Baylor College of Medicine collaborated with the clinical virology lab at University of Washington and virologists in Germany to study evaluate heart tissues from 48 consecutive pediatric patients (< 18 years) with dilated cardiomyopathy (DCM) but not acute myocarditis, as well as 10 patients who died from non-cardiac causes and had heart tissue examined at autopsy. Of the 48 patients with DCM, 4 died and had autopsies and 44 underwent a heart transplant and therefore had explanted heart tissue available for examination. Real-time PCR or RT-PCR assays for enteroviruses, adenoviruses, parvovirus B19 and HHV-6 were used to detect the presence of viral nucleic acid in myocardial tissue. Nucleic acid from parvovirus B19 was found in 17%, from HHV-6B in 8%, from enteroviruses in 3% and from both parvovirus B19 and HHV-6B in 2%. No cases of HHV-6A were detected. Among the 10 control subjects, one subject had enteroviral nucleic acid.
The heart transplant patients were followed for an average of 5 years, with recurrent endomyocardial biopsies performed, and An immunofluoresent assay was used to detect late viral antigens and was positive for parvovirus in 17% and for HHV-6B in 7%. A positive result for late antigens indicates active viral replication at the time of the biopsy. The positives were confirmed using RNA in situ hybridization.
Survival analysis found no significant difference for graft loss between virus-positive and virus-negative groups. However, survival analysis between PVB19 and HHV-6 revealed that those with PVB19 were significantly more likely to experience graft loss than those who were HHV-6B positive (Figure 1).
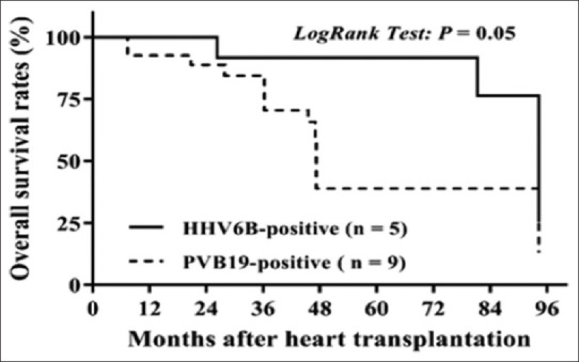
Figure 1: Kaplan-Meier survival graph comparing HHV-6B+ vs. PVB19+ overall survival
Survival analysis found no significant difference for graft loss between virus-positive and virus-negative groups. However, survival analysis between PVB19 and HHV-6 revealed that those with PVB19 were significantly more likely to experience graft loss than those who were HHV-6B positive (Figure 1).
An intriguing finding of this study is the presence of virus in the biopsy specimens from some of the donor hearts: since the myocardial tissue from the donors at the time of transplantation could not be examined, it is unclear whether the source of the virus was the donor heart or residual viral reservoirs in the recipients.
Read the full article: Das 2020