
A distinctive maculopaular pattern involving the acral areas and sometimes the trunk.
Several viral and bacterial infections have classical, typical rashes (exanthems): for example, measles, scarlet fever, rubella, erythema infectiosum, exanthem subitum, and chickenpox. But some exanthems are atypical.
Investigators in Pavia, Italy, collected 9 carefully-characterized patients with atypical rashes and HHV-7 infections, seen in their practice in the course of four years. The 9 cases did not include pityriasis rosea (a characteristic exanthem that also has been linked to HHV-7). In these patients, the rash had suddenly appeared, and involved a substantial area of their skin and disappeared with the clearance of HHV-6 viremia. Several patients had involvement only in the distal limbs, an uncommon location for most exanthems.
In all 9 cases, HHV-7 DNA was detected in plasma by RT-PCR, and subsided as the exanthem subsided. The median viral load was 1300 copies/mL of plasma. In addition, in all 9 cases there was no DNA or serologic evidence of streptococcal infection, syphilis, Mycoplasma pneumoniae, EBV, HCMV, VZV, HIV, parvovirus B19, HHV-6A/B or Coxsackievirus. None of the cases was immunocompromised, although several had diabetes and one had celiac disease.
In all 9 cases, the rash has a maculopapular pattern that always involved the acral areas—arms/hands, legs/feet, ears and nose—and often also the trunk. Two patients had fever, and 7/9 had a prominent itch. The appearance of the rash is shown in Figure 1.

The histopathological exam was available for four patients, revealing an epidermal mild spongiosis, lymphocyte exocytosis and a superficial, perivascular and interstitial infiltrate composed mainly of lymphocytes. Details on the 9 cases are displayed in Table 1, below.
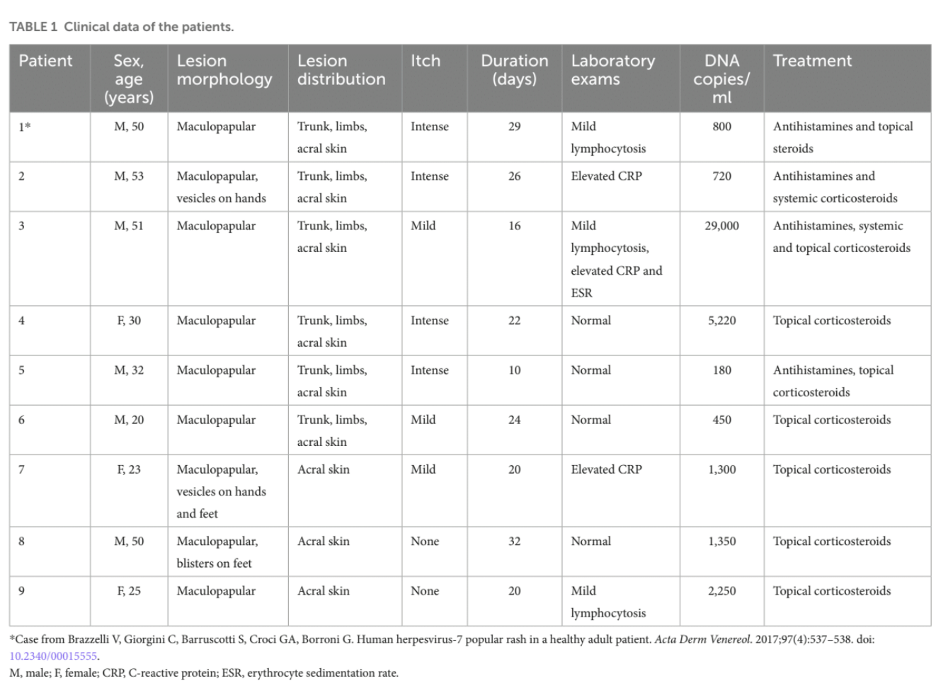
Treatment with antihistamines and topical and systemic corticosteroids promptly resolved the rash in all cases. The authors explain that antiviral drugs were not used, in part because acyclovir and ganciclovir are not effective in vitro against HHV-7 (Yoshida 1998, De Clercq 2001) and because cidofovir and foscarnet, which are effective, can have significant side effects, including nephrotoxicity.
The authors recommend that testing for HHV-7 be considered in an adult patient with a maculopapular rash prominent in the acral regions.
Read the full article: Michelerio 2024