
Studies from Europe have indicated that acute myocarditis often has a viral cause, and that HHV-6 and parvovirus B19 are two of the most common viral agents found in diseased myocardial tissue (Seitz 2022, Kühl 2005, Elsanhoury 2022, Khatami 2022, Reddy 2017). A new study from a single center in South Africa finds that the prevalence of various putative viral causes of myocarditis may be lower than what has been reported in biopsy studies in Europe.
The investigators enrolled 102 consecutive patients over 4 years in whom acute myocarditis was suspected. Each patient was systematically evaluated with symptom questionnaires, electrocardiograms, blood tests (such as cardiac troponins), trans-thoracic echocardiogram, cardiac MRI (CMR) and endomyocardial biopsy (EMB).
Of 102 patients with clinically suspected acute myocarditis, the diagnosis was confirmed by internationally-recognized criteria in 82 (80%). The presence in endomyocardial biopsy tissue of DNA and RNA from various viruses was assessed using nucleic acid amplification techniques; immunohistochemistry for viral antigens was not reported. The viruses examined included adenoviruses, influenza viruses, parainfluenza viruses, human coronaviruses, human enteroviruses, respiratory syncytial viruses human bocavirus (a recently-discovered member of the parvovirus family), human herpesviruses 1 and 2, human cytomegalovirus, Epstein-Barr virus, HHV-6 and parvovirus B19.
The presence of viral nucleic acid in biopsies from people with acute myocarditis and those with suspected but unconfirmed myocarditis are shown in the table below:
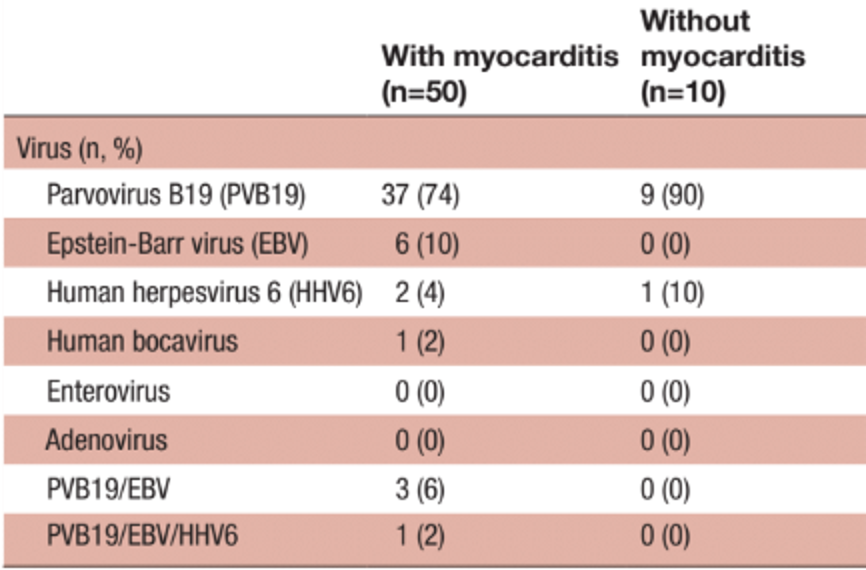
Of the 60 patients with biopsies, 50 were confirmed to have acute myocarditis; 10 did not have myocarditis, but did have other signs of cardiac disease. 37 of the 50 (74%) of the EMB confirmed myocarditis cases were positive for parvovirus B19; however, 9 of 10 (90%) who had cardiac issues that did not meet the definition of myocarditis also were positive for parvovirus B19. No cardiac tissue from healthy controls (autopsies from people experiencing non-cardiac-related death) was performed.
The strength of this study is its recruitment of a large number of consecutive patients and the systematic evaluation of each patient, including biopsies of myocardial tissue.
Unfortunately, no data are presented in this paper regarding the use of positive or negative controls and, hence, the sensitivity and specificity of the assays used. The results were not quantitative (eg. DNA copies per million cells) and no in situ hybridization or immunohistochemistry examination of viral antigens was conducted to determine cells they were infecting—myocardial cells, infiltrating leucocytes, leucocytes within blood vessels or other cells. Thus, the study does not provide information on the cell types infected by the viruses producing a positive nucleic acid signal, nor does it distinguish latent versus active/reactivated infection in the diseased tissue.
Read the full-article: Hassan 2022