SARS CoV-2 may lead to the activation of persistent herpesviruses in heart tissue.
In the past 20 years, improved molecular technologies for identifying viral nucleic acid and proteins in cardiac muscle have refined and expanded an understanding of viral infection of the heart muscle, and its role in chronic heart disease. A recent review article provides a good summary of the recent literature.
The review highlights the frequency with which parvovirus B19 nucleic acid and proteins are found in cardiac muscle, both diseased and healthy muscle. However, there is considerable evidence that the virus can cause both acute myocarditis and some cases of chronic myocardial disease. The same is true of Cocksackie B virus, although less frequently, and of adenoviruses very infrequently.
Among the herpesviruses, the evidence of virally-induced pathology is greatest for HHV-6, although there also is some evidence that EBV and (very occasionally) CMV can damage heart muscle. HHV-6 is implicated in 10-22% of patients with cardiac dysfunction (such as impaired ejection fraction of the heart ventricles), as shown in Figure 1.
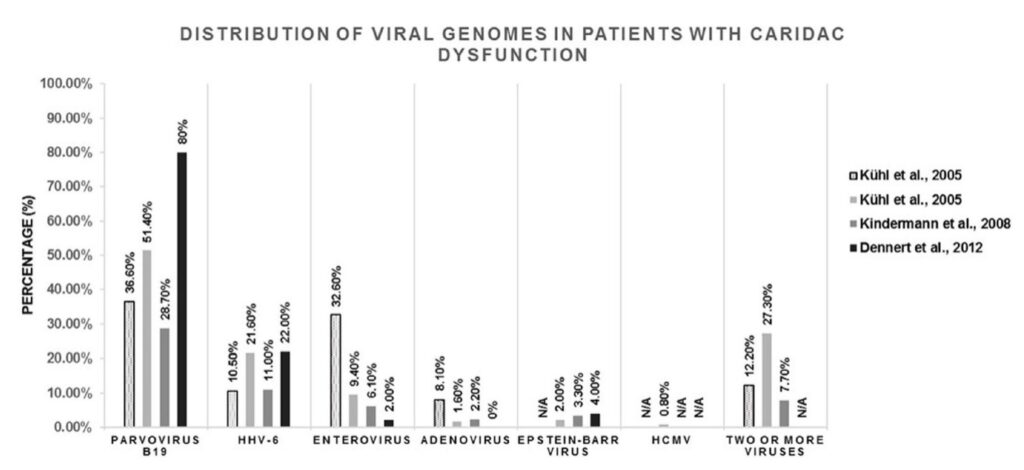
Figure 1. Frequency of finding viral genomes in human endomyocardial samples obtained from patients with cardiomyopathy (dilated cardiomyopathy or myocarditis). The amount of parvovirus B19, HHV-6, Enterovirus, Adenovirus, Epstein-Barr virus, HCMV or multi-viral presence (two of more viruses present in one endomyocardial sample) found in each individual study is shown as a percentage (%) in the respective population.
This review highlights the growing recognition that HHV-6 likely causes some cases of chronic cardiac muscle dysfunction (cardiomyopathy), and places this virus in the context of several other viruses that likely are similarly capable of causing such chronic myocardial disease.
The authors note that EBV and HHV-6 have both been shown to reactivate in patients with SARS-CoV-2, and that this may contribute to the myocardial damage often seen following severe acute infection with SARS-CoV-2. They recommend studies of EBV and HHV-6 reactivation in post-acute COVID patients with apparent myocardial damage.
Read the full article: Badrinath 2022