The clinical picture is very similar to HHV-6B encephalitis.
HHV-7 is a common cause of febrile seizures in children, as is HHV-6B, causing roughly 17% of febrile seizures in young children (Ward 2005).. However, reports of HHV-7 encephalitis in immunocompetent patients are rare.
One reason for this is that HHV-7 is not included in standard testing protocls, and it is not one of the fourteen pathogens in the BioFire FilmArray Meningitis/Encephalitis panel used widely for cerebrospinal fluid analysis.
A 2022 case report and literature review of a half dozen similar cases noted that HHV-7 encephalitis, although rare in the immunocompetent, did occur and could be severe and associated with seizures (Li 2022).
A new case report provides strong evidence of HHV-7-associated encephalitis in an immunocompetent 17-year-old male. The individual had been healthy, although he reported heavy use of marijuana. One morning he awakened with headache and abdominal symptoms, and later that day began to have repeated seizures.
On arrival at the hospital, he was treated with anticonvulsants, and placed on a ventilator. While the seizures finally abated, on regaining consciousness he was disoriented and confused. His initial laboratory test results included:
- A mild leukocytosis, predominantly due to increased numbers of lymphocytes and monocytes;
- Negative test results for HIV, syphilis and respiratory viruses;
- Normal metabolic panel and blood gases;
- Normal head CT scan;
- Negative blood cultures;
- Toxic screen testing that revealed no evidence of substance abuse;
- Negative results for autoimmune encephalitis antibodies.
On day 2 of hospitalization, however:
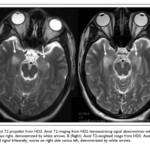
- A non-contrast MRI scan revealed FLAIR signal in bilateral mesial temporal lobes extending into parahippocampus and thalamus;
- EEG showed seizure activity in the R temporal region;
- Spinal fluid revealed increased numbers of lymphocytes, but PCR testing was negative for Herpes simplex virus-1/2.
Despite the negative test, the patient was started on acyclovir treatment. There was no improvement for several days. The results of repeat lumbar puncture on day 8 were unchanged. Repeat MRI scans showed worsening of the previous abnormalities. An MRI scan performed on hospital day 5 is shown below:
On day 13, the patient greatly improved, returning to baseline function.
Following discharge, spinal fluid testing for multiple viruses capable of causing encephalitis were positive only for HHV-7.
In this case of encephalitis—characterized by seizures with impaired consciousness and cognition—diagnostic testing ruled out many possible explanations and ultimately revealed that HHV-7 was the likely cause of encephalitis. The clinical presentation was similar clinically and radiographically to cases of HHV-6B encephalitis in immunocompromised people.
While the patient is described as “immunocompetent”—because of the absence of medical conditions or treatments that would have made him immunocompromised—it may well be that otherwise healthy young adults who develop encephalitis caused by HHV-6 or HHV-7 have some as-yet-unidentified immunological vulnerability that has been inherited or is due to environmental or lifestyle exposures (such as substance abuse).
Read the full article: Lynch 2023