HHV-6A was the most common virus identified, but was not linked to worse outcomes compared to other viral infections.
Reactivation of HHV-6B is frequently seen in hematopoietic cell transplantation (HCT). Past studies of “HHV-6 reactivation” in solid organ transplantation, like kidney transplantation, have found evidence of reactivation in 23-55% of patients, with uncertain consequences for the clinical outcome.
Investigators from several institutions in Berlin, Germany, performed serial, longitudinal studies in 93 patients before and after kidney transplantation. Serial whole blood samples were examined for the presence and viral load of DNA to HHV-6A, HHV-6B, CMV, EBV and BK virus (BKV) by qPCR using the RealStar HHV-6 kit from Altona Diagnostics that differentiates between HHV-6A and HHV-6B. Patients with reactivation of HHV-6A were not more likely to also have reactivation of CMV, EBV or BKV, as shown below.
The study detected reactivation (>250 copies/ml whole blood) of HHV-6A in 51.6% of patients; HHV-6B in 6.5%; BKV in 29.2%, CMV in 27.7% and EBV in 7.7%. HHV-6A had higher peak viral loads than other analyzed viruses.
In this study, relatively high viral loads of HHV-6A were not associated with decreased function of the renal grafts, impaired hepatic function or decreased blood counts 12 months post-transplant unlike a previous study that found an increased rate of acute graft rejection in patients with active HHV-6 infection (Caiola 2012).
However, previous studies have shown that active infection with multiple herpesvirus, including HHV-6, increase the risk of chronic allograft nephropathy and acute graft rejection (Tong 2002, Chapenko 2009). Also, biopsy studies have found that allografts containing HHV-6 and other viral DNA had significantly higher scores for interstitial fibrosis and tubular degeneration (Sebekova 2005).
Finding HHV-6A was surprising to the investigators who noted that HHV-6B is typically the dominant variant found in hematopoietic transplant cases as well as in kidney failure subsequent to DRESS/DIHS. However, these results are consistent with previous reports of prominent reactivation of HHV-6A in kidney transplant patients. Csoma et al found HHV-6A in 8/9 patients with viremia post kidney transplant. Also, at least three case reports have described kidney transplant patients who died from acute HHV-6A infections (Deborksa-Materkowska 2005, Rossi 2001, Pilmore 2009).
Finally, patients with reactivation of HHV-6A were more likely to also have reactivation of HHV-6B, although the association was not quite statistically significant; however, because of the relatively infrequent reactivation of HHV-6B, the study was underpowered to recognize the correlation as significant. Patients with reactivation of HHV-6A were not more likely to also have reactivation of CMV, EBV or BKV, as shown in the Figure.
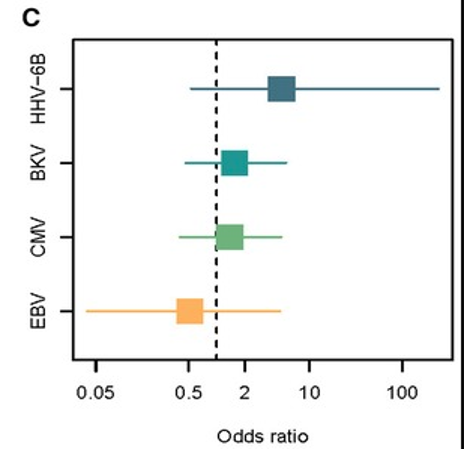
Figure 1: Odds ratios that a person with reactivation of HHV-6A would also demonstrate reactivation of other viruses. Statistically significant odds ratios would not have a confidence interval that included 1.0.
Thus, there is growing evidence that reactivation of both HHV-6A and HHV-6B occurs often in solid organ transplantation; the clinical consequences of this reactivation remain uncertain, making it important to support future research addressing this question.
Read the full article: Blazquez-Navarro 2023