
Among infectious agents, HHV-6 was found to be an independent risk factor for thrombotic microangiopathy (TMA) and only HHV-6 infection was associated with TMA-related mortality.
Transplant-associated thrombotic microangiopathy (TMA) is a rare complication of hematopoietic stem cell transplantation (HSCT), thought possibly to be secondary to infection.
Ramgogal et al. of the Children’s Hospital of Pittsburgh investigated various risk factors for TMA, including HHV-6 reactivation, in a retrospective cohort of 12,369 children undergoing HSCT at multiple hospitals over 12 years. Risk factors for TMA included allogeneic HSCT, peripheral blood stem cell transplants, CMV infection, fungal infection, graft-versus-host disease (GVHD) and veno-occlusive disease, as well as HHV-6 infection. Among these various risk factors, multivariate analysis demonstrated that only HHV6 was an independent risk factor for TMA-related mortality, with a hazard ratio of 2.86. Survival curves are shown in Fig 1.
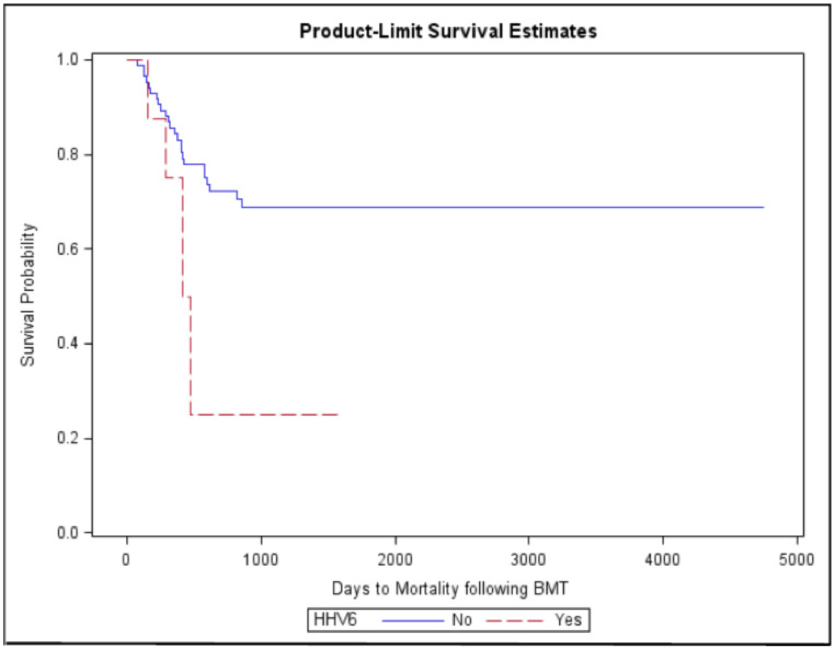
Fig 1 - Overall mortality in HSCT patients with and without HHV-6.
The mechanisms by which HHV-6 might increase the risk of TMA and TMA-related mortality are speculative and include inhibition of angiogenesis and enhanced activity of the complement cascade. A recent meta-analysis showed that HHV-6B infection is a risk factor for subsequent acute GVHD (Phan et al. 2018), which in turn is a risk factor for TMA. However, multivariate analysis revealed that HHV-6 was a risk factor for TMA independent of its ability to increase the risk of GVHD, and HHV-6 (but not GVHD) was also an independent risk factor for TMA-related mortality. Thus, it is plausible that HHV-6 may play a role in the genesis of this rare complication in people undergoing HSCT.
Read the full article: Ramgopal 2021