
Value of this observation in determining prognosis or guiding treatment remains to be studied.
Torque teno virus (TTV) is a novel non-enveloped, circular, and single-stranded DNA virus that is regarded as non-pathogenic and which has a prevalence of up to 90% in healthy and up to 100% in kidney transplant patients. Some studies have suggested that its reactivation may be linked to the reactivation of other, pathogenic, viruses that are thought to affect the outcome of kidney transplantation like human BK virus (BKV), Epstein–Barr virus (EBV), or cytomegalovirus (CMV).
A team from multiple institutions in Germany obtained blood samples from 93 kidney transplantation patients on nine occasions over the course of a year. The samples were analyzed for TTV/BKV/CMV/EBV/HHV-6A DNA load using quantitative PCR. Clinical characteristics, including graft function [glomerular filtration rate (GFR)], were collected in parallel.
The team found that all of the patients, on all occasions during the year, had detectable TTV DNA, with the level rising for the first 3-4 months, and then declining slightly over the next 9 months. After TTV, HHV-6 was the next most prevalent virus, as shown in Figure 1.
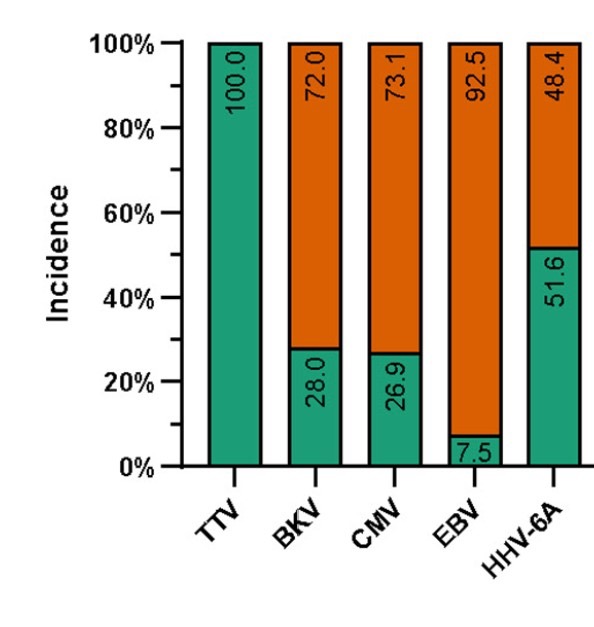
Figure 1. Prevalence (shown in green) of detectable DNA in blood from five viruses, over the course of one year following kidney transplantation.
The levels of DNA for these viruses were not correlated with estimated kidney function. However, as found by some previous investigators, patients with lower TTV loads (<5.0 cp/ml (log10)) had a higher incidence of acute rejection, in comparison to patients with a higher TTV load.
Also, patients with a lower TTV load were more likely to have reactivation of both HHV-6A and BKV, as shown in Figure 2, below. In contrast, there was no such association of TTV load with the viral loads of EBV or CMV.
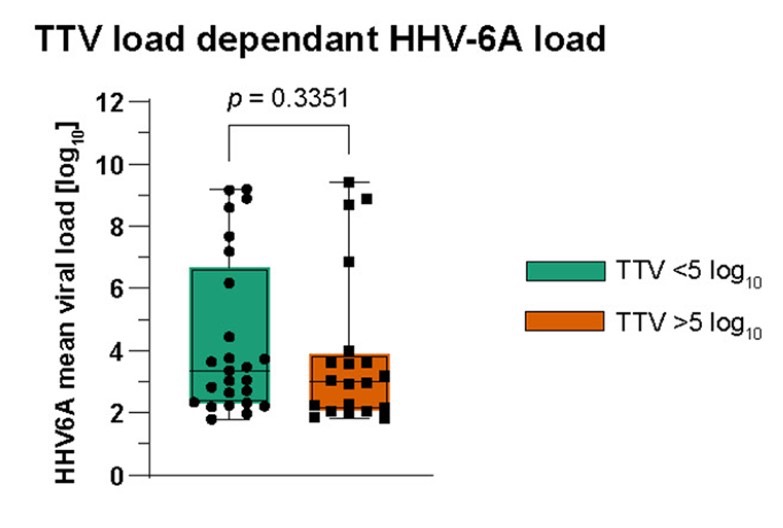
Figure 2: Patients with the lowest TTV load (in green) had higher HHV-6A loads than patients with higher TTV loads (in orange).
Did the higher HHV-6 viral loads seen in people with lower TTV loads correlate with outcomes of kidney transplantation? Previous studies have shown that active infection with multiple herpesvirus, including HHV-6, increase the risk of chronic allograft nephropathy and acute graft rejection (Tong 2002, Chapenko 2009, Sanchez-Ponce 2019.). Also, biopsy studies have found that allografts containing HHV-6 and other viral DNA had significantly higher scores for interstitial fibrosis and tubular degeneration (Sebekova 2005).
In addition, a previous study done by this same group of German investigators in 2023 found HHV-6A reactivation in 52% of 93 kidney transplant patients, but did not find HHV-6A to be associated with decreased renal graft function (Blazquez-Navarro 2023.).
One point worth highlighting: the authors don’t mention inherited chromosomally integrated HHV-6 (iciHHV-6) in the paper. However, their data indicates at least 11 of the 48 HHV-6+ patients had viral loads of greater than 1 million copies per ml or greater, values that are generally considered more likely to reflect iciHHV6 than reactivation of HHV-6.
In summary, this study suggests that there may be an interaction between the reactivation of TTV and HHV-6A in patients undergoing kidney transplantation. Whether measurement of these viral loads has prognostic value, or helps clinicians make decisions about immunosuppressive therapies, will require larger studies.
Read the full article: Rosiewicz 2024