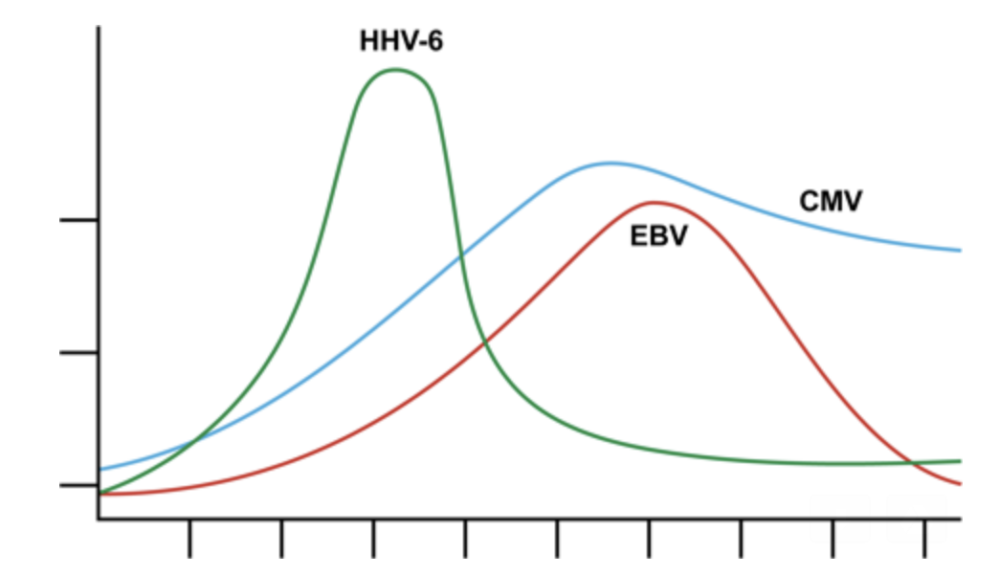
A group at Fred Hutch Cancer Research Center studied the kinetics of viral reactivation for HHV-6B, CMV, BKV, AdV, and EBV in weekly plasma samples from 404 patients after hematopoietic cell transplant (HCT). HHV-6B reached maximum levels earlier (median 3 weeks) than all other viruses analyzed, and had the shortest interval between detection and end-organ disease, suggesting pre-emptive therapy for HHV-6 based on viral load thresholds – a strategy currently used for many other viruses, including CMV and EBV (which take 2-3 weeks to reach peak viral loads) could be largely ineffective for HHV-6.

Source: Hill 2017C
HHV-6B detection lasting <4 weeks was distinctly characterized by rapid progression to peak viral load, followed by rapid decay. In contrast, when HHV-6B detection lasted >4 weeks, patients experienced early peaking of viral load followed by only a slight decay and an extended plateau period of lower level detection.
Only CMV and HHV-6B were associated with increased overall mortality between days 101-365. For all viruses except HHV-6B, higher cumulative “Area Under the Curve” (AUC) was found to increase risk for overall mortality through day 100.
End-organ disease, which occurred in 34 patients, was also found to be temporally related to onset of persistent (>1 week) viremia for all viruses. End organ disease observed in this study included 24 cases of CMV (20 gastrointestinal, 4 pulmonary), 6 cases of HHV-6B (central nervous system), 5 cases of AdV (2 gastrointestinal, 2 pulmonary, 1 gastrointestinal and pulmonary), and 1 case of EBV (central nervous system).
The authors conclude that a “one size fits all” approach may not be the most effective treatment strategy and that their findings could help optimize unique treatment strategies for each virus. For example, the group suggests that HHV-6B end-organ disease may be most appropriately addressed prophylactically given that HHV-6B episodes were found to have the highest initial viral load and reached maximum levels within one week of onset, with a very short period between plasma detection and end-organ disease (median 5 days) when compared to other viruses (median >7 days). They pointed to the failed Japanese trial of preemptive therapy to prevent HHV-6B encephalitis as evidence that prophylaxis may be required due to the rapid onset of HHV-6B encephalitis after the first evidence of plasma viremia (Ishiyama 2011).
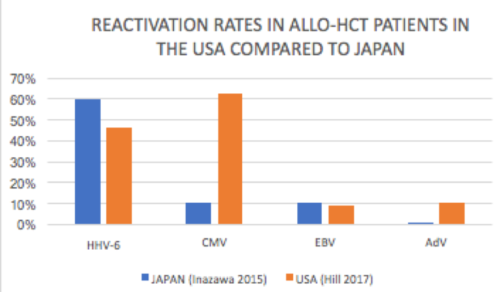 CMV, found in 59% of the 404 patients tested, was the most frequently reactivated virus in the Fred Hutch study compared to 47% for HHV-6 and 9% and 10% for EBV and adenovirus respectively. On the other hand, in Japan, a similar study of 105 patients found that HHV-6 had the highest reactivation rate at 60%, followed by CMV and EBV at 10.5% respectively and adenovirus at only 1% of patients (Inazawa 2015). Reactivation rates vary depending on the cell source and seropositivity for CMV.
CMV, found in 59% of the 404 patients tested, was the most frequently reactivated virus in the Fred Hutch study compared to 47% for HHV-6 and 9% and 10% for EBV and adenovirus respectively. On the other hand, in Japan, a similar study of 105 patients found that HHV-6 had the highest reactivation rate at 60%, followed by CMV and EBV at 10.5% respectively and adenovirus at only 1% of patients (Inazawa 2015). Reactivation rates vary depending on the cell source and seropositivity for CMV.
Read the full paper: Hill 2017C