HHV-6B reactivation after hematopoietic stem cell transplantation (HSCT) causes approximately 35% of CNS infections post-allogeneic-HSCT. Retrospective analysis of 16 HSCT patients with HHV-6 encephalitis and/or myelitis revealed that hyponatremia- low serum sodium levels- was associated with HHV-6 encephalitis, but not myelitis, and has the potential to be used to diagnose or predict the onset of the disorder.

Sodium levels drop before the onset of HHV-6 encephalitis but not before HHV-6 myelitis.
Source: International Journal of Hematology
Hyponatremia (Chik 2002, Kawaguchi 2013) and hypernatremia (Shimazu 2013) have been documented in patients who underwent HSCT and developed HHV-6 encephalitis, as well as in one boy with drug-induced liver injury due to HHV-6 reactivation (Fujita 2015). To further investigate the clinical significance of this phenomenon, the authors of this study compared the blood sodium levels of patients with either HHV-6 encephalitis, myelitis, or both post-transplant.
Five patients developed encephalitis, and 4 of the 5 also developed myelitis. Serum sodium decreased in all 5 at the onset of encephalitis, and the median of 129.1 mEq/L was significantly lower than that of patients with myelitis alone as well as 80 controls who had undergone HSCT but did not have HHV-6 encephalitis/myelitis. In 3 of 5 patients, hyponatremia preceded the encephalitis by 1-2 days, and serum sodium rose 1-4 days after onset. The investigators posit that HHV-6 may cause the syndrome of inappropriate secretion of antidiuretic hormone (SIADH), which can occur in association with CNS infections and is known to result in hyponatremia. They suggest that physicians should be mindful to treat both the underlying HHV-6 infection, with antivirals, and the hyponatremia by sodium supplementation. Of interest, the increasing sodium levels in the serum of the 5 hyponatremic patients in this study corresponded to administration of foscarnet at the onset of encephalitis; massive quantities of saline were given along with the antiviral in an attempt to offset the drug’s nephrotoxicity.
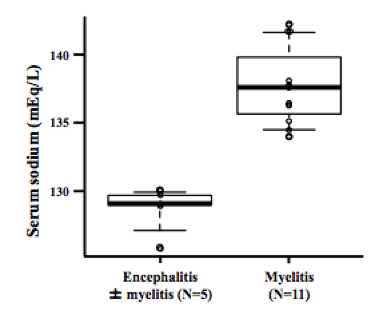
Comparison of serum sodium levels in HHV-6 encephalitis vs. HHV-6 myelitis
Source: International Journal of Hematology
Previous analysis indicates that the presence of HHV-6 in CSF positively correlates with the development of encephalitis post-transplant (Greco 2016), and immune reconstitution is linked to better outcomes in terms of complications related to HHV-6 reactivation, including graft-versus-host-disease (GvHD) (Admiraal 2017) and survival (Greco 2016). The identification of hyponatremia as a possible marker for HHV-6 encephalitis post-transplantation carries the potential to allow for more accurate and timely diagnosis, which could in turn help prevent the development of this life-threatening disorder as well as the severe neurological sequelae that follow.
For more on HHV-6 reactivation post-transplantation, visit our page on HHV-6 and Transplant Complications.
Find the full paper here: Murakami 2017.